
The information in this website is intended only for healthcare professionals. By entering this site, you are confirming that you are a healthcare professional.
The information in this website is intended only for laboratory professionals. By entering this site, you are confirming that you are a laboratory professional.
Asthma, a chronic, common condition characterized by symptoms of wheezing, breathlessness, chest tightening, and cough, is an inflammatory disorder that causes airway hyperresponsiveness and airflow obstruction.1
Uncontrolled asthma can have a profound, negative effect on a patient’s quality of life. Despite current interventions and substantial healthcare investment, approximately 250,000 people worldwide die each year from asthma; almost all these deaths being avoidable.1
Allergen sensitization is a critical component to assess when diagnosing asthma. Exposure to allergens can cause airway inflammation and increase the risk for an exacerbation.2 Guidelines suggest identifying factors that can instigate asthma, including allergens, when evaluating a patient.2 Assessing a patient’s symptom threshold by testing IgE and identifying relevant sensitizing allergens can help clinicians make the most accurate diagnosis and treatment plan.2
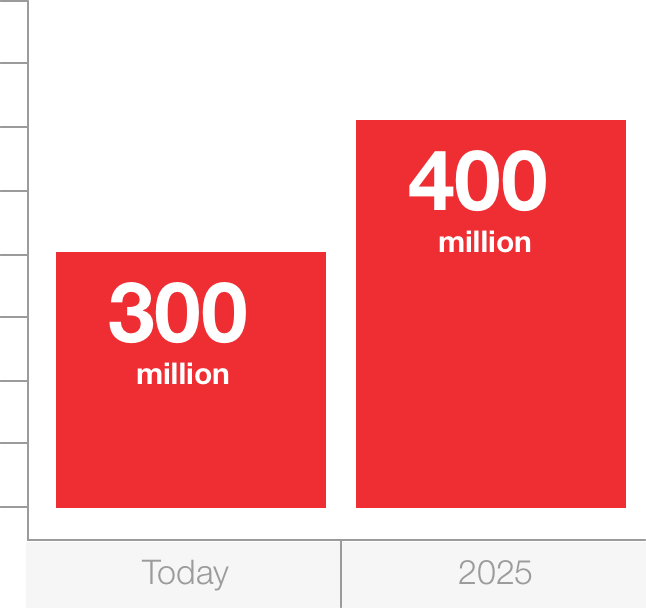
Asthma affects approximately 300 million people in the world,1 and is estimated to affect 400 million people by 2025.1
Several well-established guidelines exist to aid healthcare providers in creating a personalized management plan for patients with asthma:
These guidelines all recommend laboratory testing to determine which factors are contributing to a patient’s asthma. These could include sensitizations to perennial, seasonal, indoor, or environmental allergens, which can be assessed by the results of specific IgE testing. Skin prick tests (SPT), serological tests, or a combination of both can increase a provider’s diagnostic certainty when added to an allergy-focused patient history.3 Having the ability to rule in or out sensitization to certain allergens can help providers arrive at the correct diagnosis sooner and can greatly assist in the development of a personalized management plan that yields the greatest outcomes for patients.4
Explore available assays for identifying aeroallergen sensitization
Developing an effective management plan that is specific to the pathogenesis of the patient’s disease begins by understanding just that. If allergens are the root cause, it is critical that a provider understand which ones the patient is sensitized to. That can help him or her choose among the available management strategies, such as allergen avoidance or pharmacologic treatments, to create the most appropriate management plan.
The identification of allergens is important not only to the diagnosis and management of asthma but to other conditions and diseases as well.
The impact of allergy on asthma is staggering:
Children with asthma and concomitant food allergy have a seven times higher risk for life-threatening asthma exacerbations5,6
Patients with asthma, allergen, exposure, and viral infection face a nearly 20-fold increased risk for hospitalization compared to patients with allergies alone7
Patients with asthma plus an allergy to peanuts or tree nuts are at an increased risk for fatal anaphylaxis8
It is also important to remember that having specific information allows the clinician to better educate his or her patient on the connection between allergy and asthma. The clinician can also help the patient better understand his or her treatment and how to take a more active role in treatment. This enhanced engagement has been shown to strengthen the provider-patient relationship and increase adherence, which is tied to enhanced outcomes.2
Learn more about the systems and assays available to your lab >
Pawankar R, Holgate ST, Canonica GW, et al. World Allergy Organization (WAO) White Book on Allergy. 2013. World Allergy Organization Website. Available at http://www.worldallergy.org/UserFiles/file/WhiteBook2-2013-v8.pdf. Accessed November 2017.
US Department of Health and Human Services. National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma. 2007. https://www.nhlbi.nih.gov/files/docs/guidelines/asthgdln.pdf. Accessed November 2017.
British Thoracic Society. British guideline on the management of asthma. 2016. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-asthma-guideline-2016/. Accessed November 2017.
Duran-Tauleria E, Vignati G, Guedan MJ, et al. The utility of specific immunoglobulin E measurements in primary care. Allergy. 2004;59(Suppl 78):35-41.
Roberts G, Patel N, Levi-Schaffer F, et al. Food allergy as a risk factor for life-threatening asthma in childhood: a case-controlled study. J Allergy Clin Immunol. 2003;112:168-174.
Liu AH, Jarmillo R, Sicherer S, et al. National prevalence and risk factors for food allergy and relationship to asthma: results from the National Health and Nutrition Examination Survey 2005-2006. J Allergy Clin Immunol. 2010;126:798-806 e13.
Murray CS, Poletti G. Kebadze T, et al. Study of modifiable risk factors for asthma exacerbations: virus infection and allergen exposure increase the risk of asthma hospital admissions in children. Thorax. 2006;61:376-382.
Lomas JM, Järvinen KM. Managing nut-induced anaphylaxis: challenges and solutions. J Asthma. 2015;8:115-123.
Some products may not be available to you, and indications may differ from your original region's approved use.



